To schedule a consultation with Dr. Most, please call (650) 736-3223.
Serving patients from Palo Alto, San Francisco, San Jose, and throughout the Bay Area.
Dorsal Hump
Management of the Osseocartilaginous Dorsum (Educational Overview)
This page summarizes surgical concepts for trainees and colleagues; it is not intended as medical advice.
Conventional Hump Resection
The conventional approach to dorsal hump correction begins with thorough preoperative analysis. Determining the relative contribution of bone versus cartilage — as well as patient-specific anatomic features like radix depth and supratip break — informs the surgical plan.
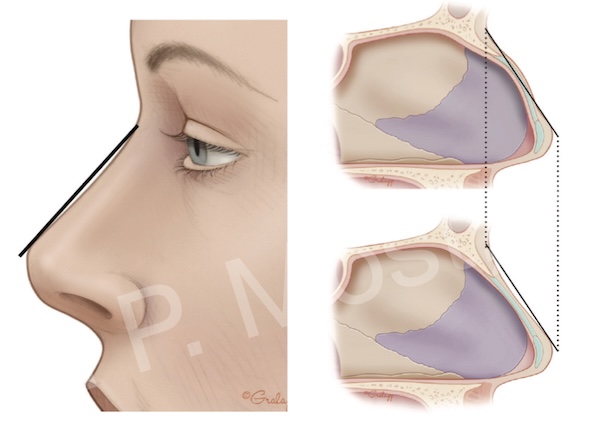
Figure 7-3: Key relationships used during dorsal profile assessment.
Anatomic understanding of the osseocartilaginous vault is essential. The nasal bones taper inferiorly and are fused with the upper lateral cartilages along the dorsal septum. This continuity forms the dorsal roof.
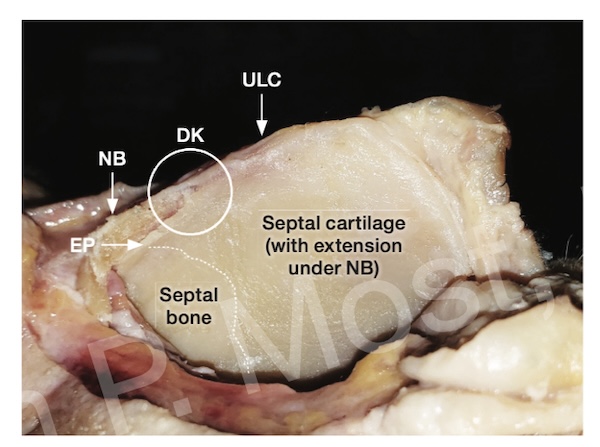
Figure 7-6: Fused cartilaginous-bony segment that defines the dorsal aesthetic lines.
Traditional hump reduction entails resecting both bony and cartilaginous elements. Access is gained via subperichondrial and subperiosteal dissection, allowing for controlled exposure and protection of adjacent soft tissue structures.
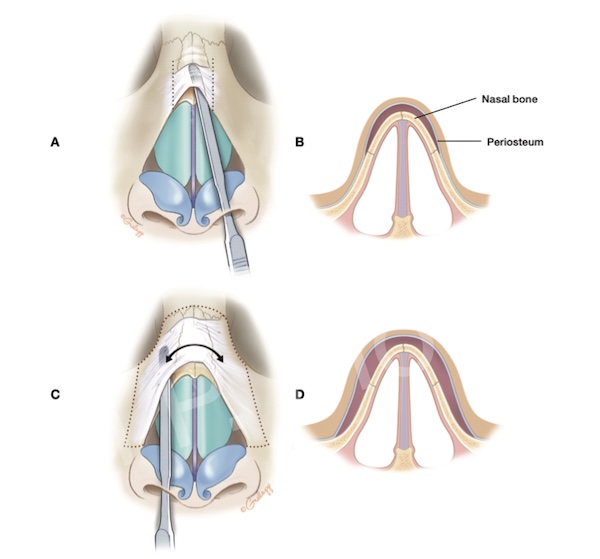
Figure 7-10: Periosteal dissection for safe access to bony vault during traditional hump resection.
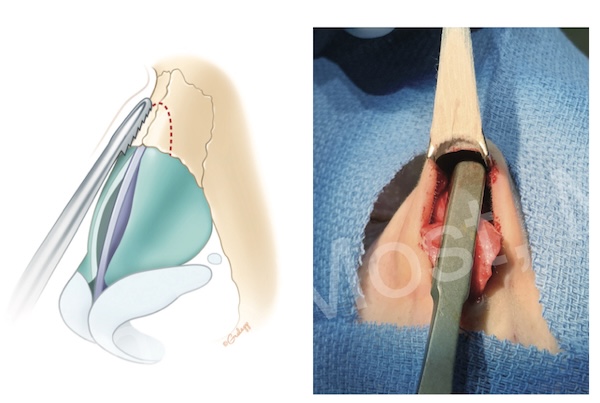
Figure 7-12: Bone rasp used to smooth residual irregularities after hump resection.
There are various methods for cartilage reduction. The method often used by the senior author is ‘component reduction’, whereby the cartilaginous vault and bony vault are addressed separately. ‘En bloc’ resection (not shown) involves removal of the bone and cartilage as one unit.
However, once the hump is removed, the continuity of the dorsal vault is lost — creating an “open roof” deformity. To address this, osteotomies are often required and performed to mobilize and medialize the nasal bones, restoring the dorsal width. Spreaders (grafts or flaps) are often added to restore internal valve function and reconstruct dorsal support.
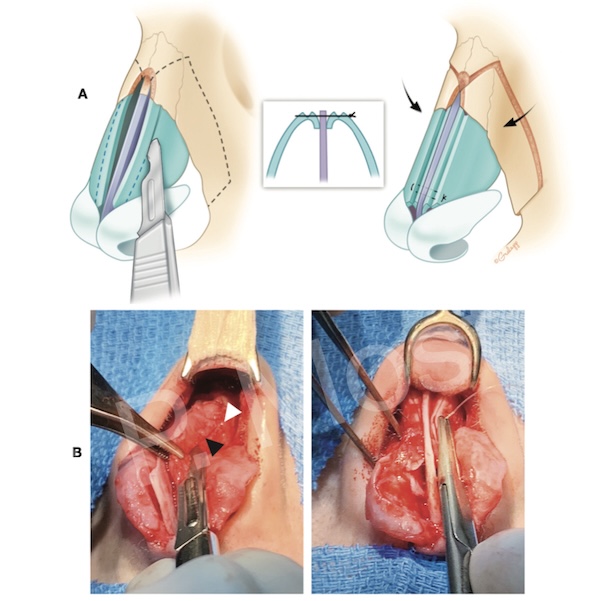
Figure 7-21: Postoperative appearance with dorsal narrowing after osteotomies and autospreader flaps.
Clinical Outcomes of Conventional Resection

Figure 7-24: Example of patient with conventional hump resection.

Figure 7-25: Example of patient with conventional hump resection.

Figure 7-27: Example of patient with conventional hump resection.
Dorsal Preservation: Principles and Evolution
Dorsal preservation (DP) rhinoplasty offers an alternative to the standard hump takedown. Instead of resecting the dorsum, this technique maintains the native dorsal roof and aesthetic lines by lowering the entire dorsum en bloc. It preserves keystone-area integrity and avoids disruption of the ULC-septal attachments, reducing the need for grafting or reconstruction.
The foundation for this approach dates back more than a century, but recent refinements have made it widely accessible. Dr. Most has published extensively regarding this technique, and in particular, adaptation of the method to structural rhinoplasty, hence the term ‘structural preservation rhinoplasty’.
Figure 8-1: Cross-section comparing dorsal preservation (right) and traditional resection (left).
The two most common preservation techniques are push-down and let-down.
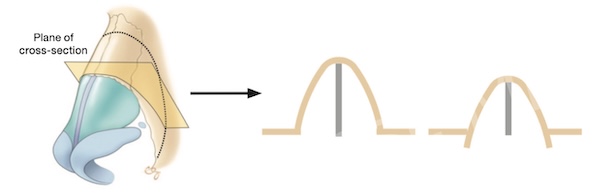
Figure 8-4: Push-down technique using subdorsal septal strip resection.
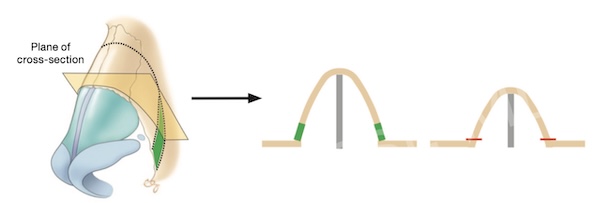
Figure 8-5: Let-down technique with wedge resections at nasal base.
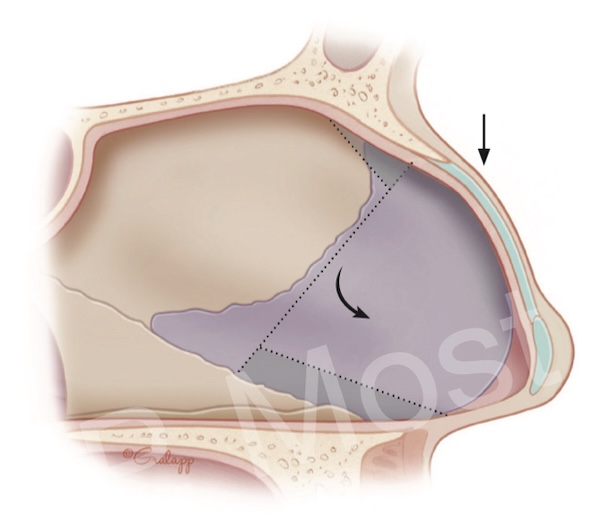
Figure 8-9: Cottle method showing triangular septal strip removal.
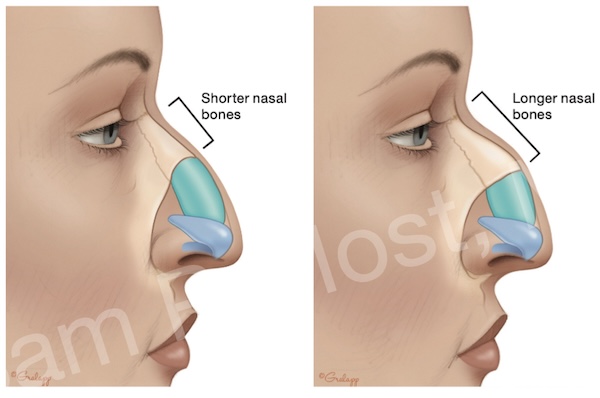
Figure 8-14: Longer nasal bones favor better outcomes in dorsal preservation.
Subdorsal Modification and Most’s Modified Technique
Effective dorsal preservation depends on subdorsal modification. One approach that has gained prominence is Dr. Most’s Modified Subdorsal Strip Method (MSSM). This involves selective resection of a narrow triangular strip beneath the dorsum to allow controlled lowering, while preserving the dorsal roof.
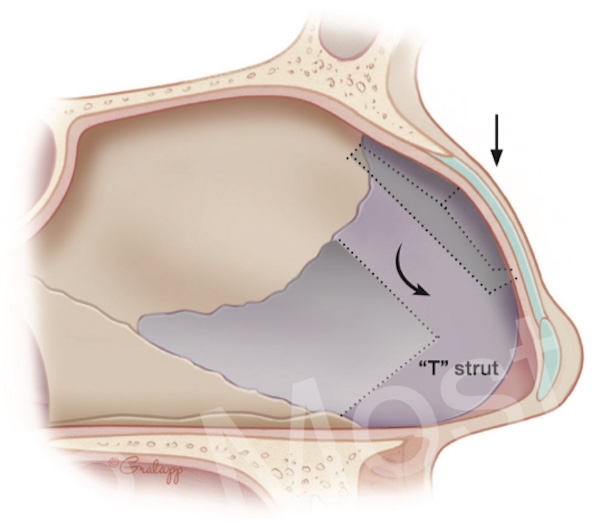
Figure 8-16: Triangular subdorsal resection with optional 'T' strut for support.
Preservation of soft tissue and mucosal flaps is critical to avoiding instability or airway compromise. This method reduces the risk of dorsal irregularities and avoids the need for dorsal grafts or spreaders.
Clinical Outcomes of Dorsal Preservation

Figure 8-25: Example of patient with DPR (MSSM).
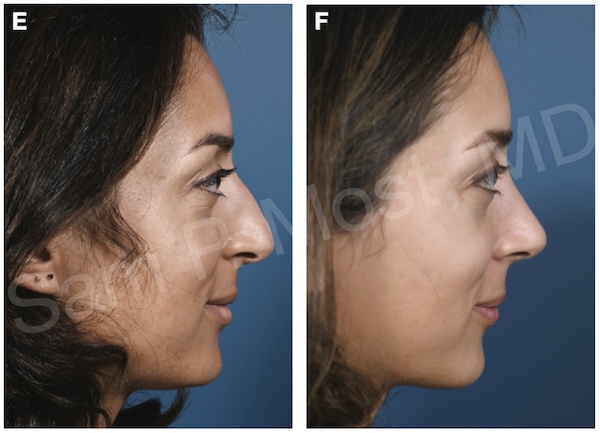
Figure 8-26: Example of patient with DPR (MSSM).

Figure 8-28: Example of patient with DPR (MSSM).
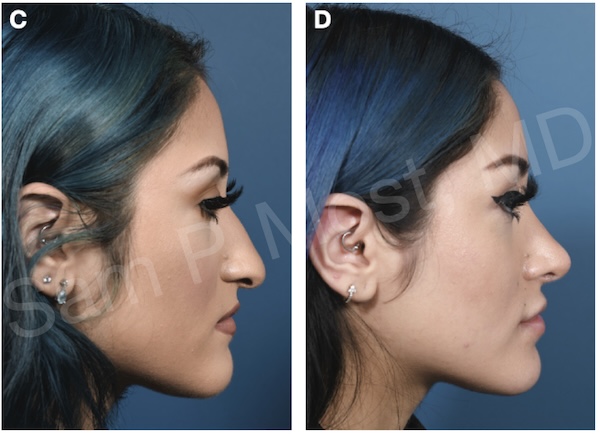
Figure 8-29: Example of patient with DPR (MSSM).
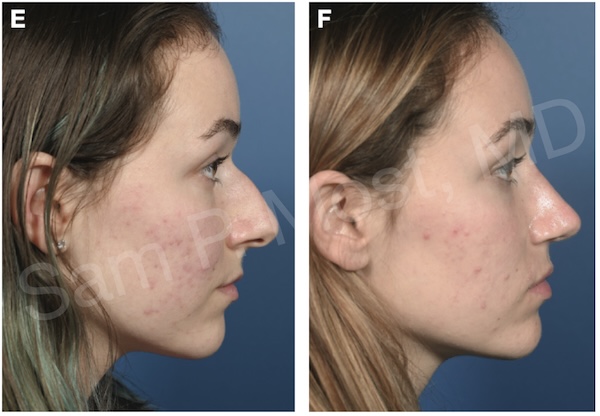
Figure 8-31: Example of patient with DPR (MSSM).
Summary
The decision between conventional resection and dorsal preservation depends on multiple factors: nasal anatomy, skin thickness, dorsal contour, and surgeon expertise. Traditional hump takedown remains effective, especially in complex or asymmetric cases. However, preservation rhinoplasty — particularly using refined techniques like the Modified Subdorsal Strip — allows for natural outcomes with reduced need for grafting and fewer structural disruptions.
By understanding and mastering both paradigms, the rhinoplasty surgeon gains greater flexibility in tailoring procedures to each patient’s needs, optimizing both form and function of the nose. Note that not every patient is a candidate for dorsal preservation, and good outcomes can be achieved with both conventional hump resection and dorsal preservation methods.