To schedule a consultation with Dr. Most, please call (650) 736-3223.
Serving patients from Palo Alto, San Francisco, San Jose, and throughout the Bay Area.
Nasal Obstruction
Surgical Concepts in Functional Rhinoplasty
This page summarizes surgical concepts for trainees and colleagues; it is not intended as medical advice.
Nasal obstruction is one of the most common complaints in both functional and cosmetic rhinoplasty consultations. Patients may describe difficulty breathing through one or both sides of the nose, worsened by exercise, sleep, or environmental irritants. Because nasal breathing is essential to comfort, athletic performance, and quality of life, identifying and treating the specific cause of obstruction is crucial.
Dr. Most takes a comprehensive and individualized approach to nasal obstruction, combining medical evaluation with surgical expertise to treat both internal and external causes of airway compromise. The following is distilled from the textbook, Comprehensive Rhinoplasty: Structural and Preservation Concepts.
Evaluating the Patient: Beyond the Nose Alone
The first step in treating nasal obstruction is careful diagnosis. Not all breathing problems are structural, which is what we can treat surgically. Environmental allergies, chronic rhinitis, or sinusitis may mimic mechanical blockage. That’s why a full history and examination—including allergy testing, endoscopy, and sometimes imaging—are essential to rule out reversible or non-surgical contributors.
When a structural cause is confirmed, obstruction is typically divided into static and dynamic contributors (see Figure 3–2).
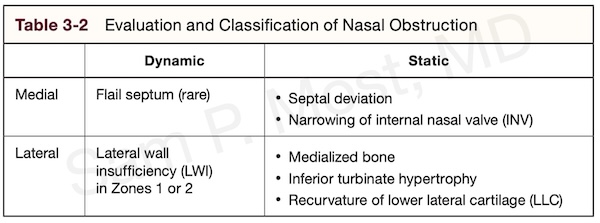
Figure 3–2. Static and dynamic contributors to nasal obstruction.
The Role of the Septum and Turbinates
A deviated septum—where the cartilage and/or bone dividing the nasal passages is crooked—is one of the most common structural contributors to obstruction. Some deviations are visible externally; others are internal but still cause significant narrowing of the airway. Septoplasty is the procedure to straighten the septum and can be performed alone or with rhinoplasty. It does not intentionally change the shape of the nose.
Turbinates are scroll-like structures inside the nasal passage that humidify and filter air. The inferior turbinate can become enlarged due to allergies or chronic irritation. In most cases, turbinate reduction can be performed conservatively, preserving function while improving airflow.
See Figure 3–16 for an illustration of the septum and the three paired turbinates: superior (ST), middle (MT), and inferior (IT).
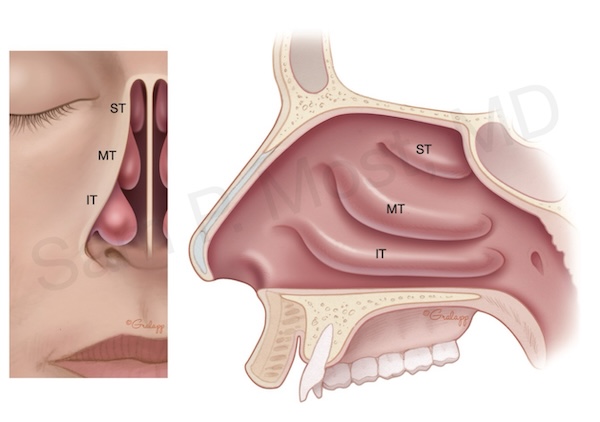
Figure 3–16. Superior (ST), middle (MT), and inferior (IT) turbinates.
Internal Nasal Valve: The “Bottleneck” of Breathing
The internal nasal valve (INV) is the narrowest part of the nasal airway and a critical point of resistance. Even small anatomical issues can result in significant obstruction. Correction may include spreader grafts or structural techniques that widen the angle and reinforce sidewall integrity.
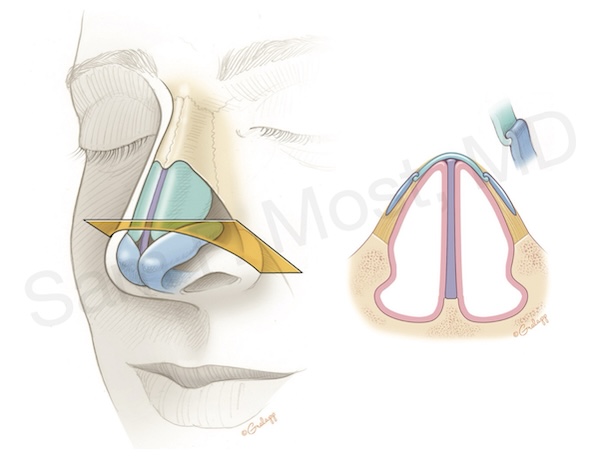
Figure 3–15. Internal nasal valve components and bottleneck.
Lateral Wall Insufficiency: Zones and Collapse
Some patients experience nasal collapse during inspiration—often due to lateral wall insufficiency (LWI), where the nasal sidewall lacks strength to remain open. Collapse is observed in Zones 1 and 2, as shown below.
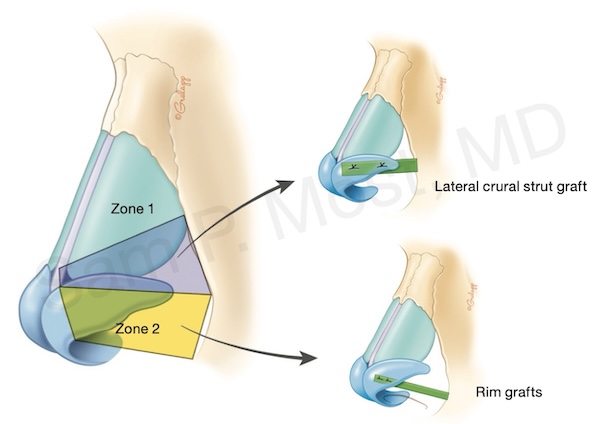
Figure 3–18. Nasal sidewall zones involved in LWI.
Septoplasty and the Modern ASR Technique
Traditional septoplasty elevates the mucosa and reshapes or removes deviated septal cartilage. Figure 5–4 shows mucosal elevation; Figure 5–5 shows the view before cartilage correction.
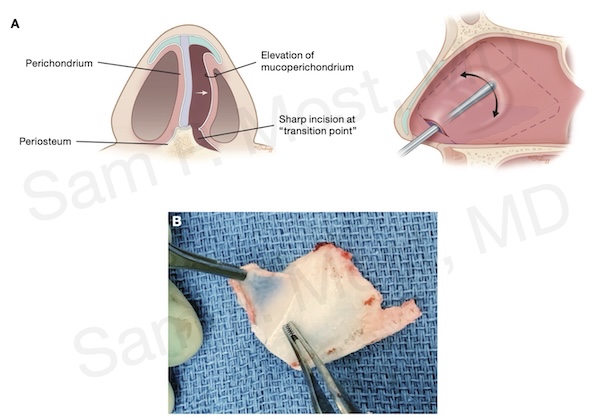
Figure 5–4. Mucoperichondrial elevation at cartilage/bone transition.
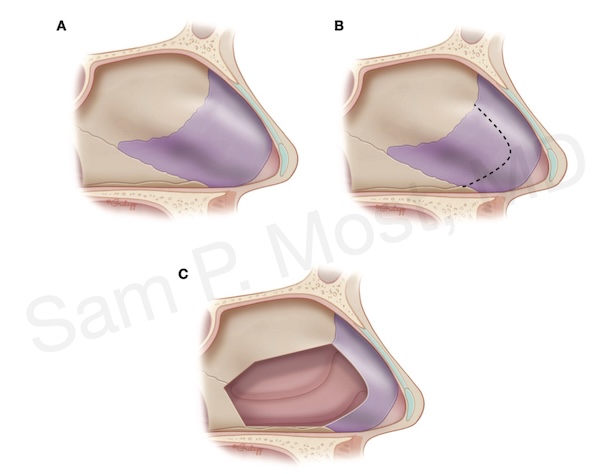
Figure 5–5. Septum view after mucosal elevation.
For more complex cases, Dr. Most uses Anterior Septal Reconstruction (ASR), a technique he published. This involves removing, reshaping, and re-implanting a cartilage construct. Figure 5–7 shows this with dorsal preservation and a base notch to lock the graft in place.
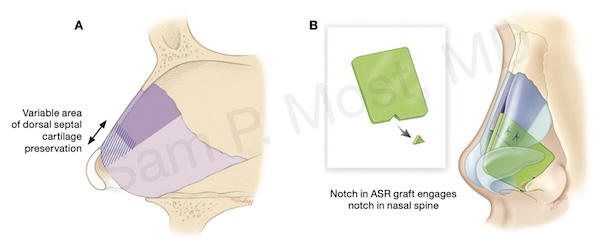
Figure 5–7. ASR diagram with locking notch and dorsal preservation.
Figure 5–6 shows a before-and-after base view where ASR corrected severe airway collapse and septal deviation.
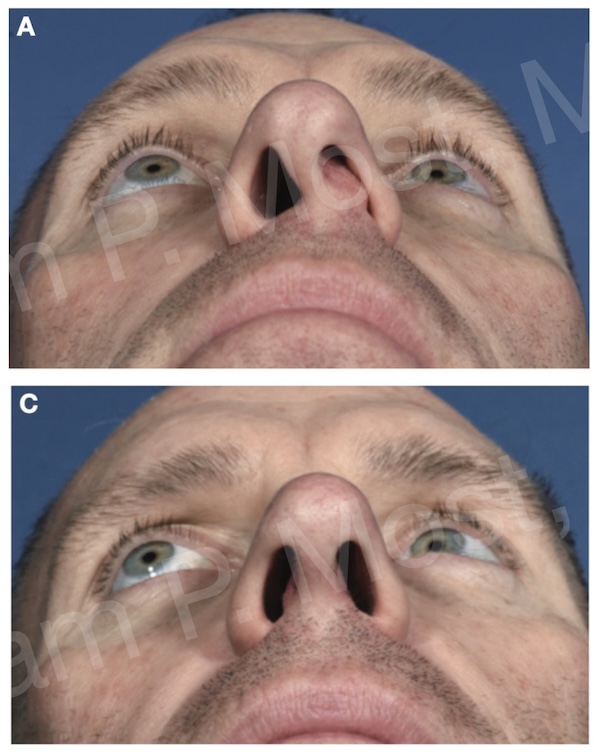
Figure 5–6. Base view pre- and post-ASR.
Cartilage Grafting and Reinforcement
Patients with INV narrowing or LWI may benefit from cartilage grafts harvested during septoplasty (or from ear/rib). Figure 5–2 shows the Posterior Quadrangular Cartilage Extension (PQCE), an important piece often preserved during harvest.
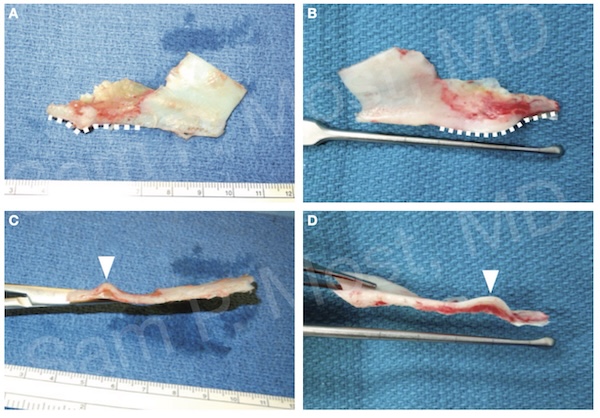
Figure 5–2. Posterior Quadrangular Cartilage Extension (PQCE).
Figure 5–10 shows septum harvest for ASR construction, and Figure 5–11 shows batten grafts used to correct severe deviation.
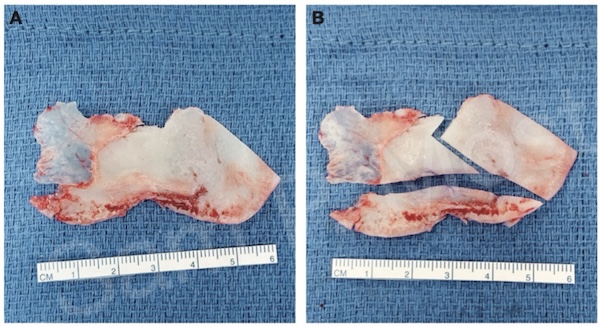
Figure 5–10. Septum harvest for ASR grafts.
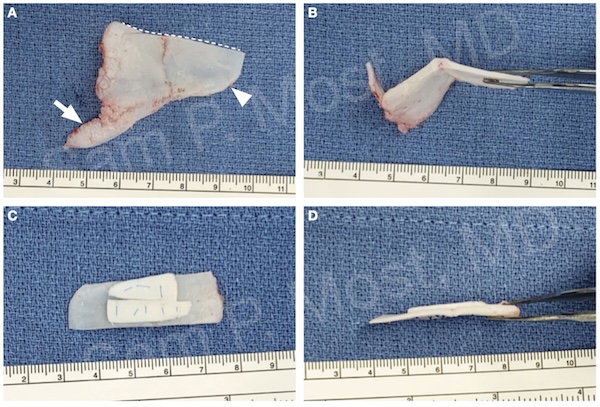
Figure 5–11. Batten graft reinforcement in severe axis deviation.
Tailored, Lasting Results
Each patient presents a unique combination of structural, dynamic, and inflammatory factors. Dr. Most’s approach prioritizes functional preservation while restoring airflow and nasal balance. Whether the issue is septal deviation, enlarged turbinates, valve collapse, or weak sidewalls — precise diagnosis and surgical planning allow for long-lasting, functional improvement.